
Case Study
The story of Covid (&) Vaccination in India
Role /
Lead Designer
UX Researcher
Duration /
5 months
Year /
Jan '21 to May '21
The role of private hospitals in vaccinating the country
India had come out of its first lockdown in a total of six phases lasting six months. There was a general restlessness among people. This was followed by the disregard for Covid-19 protocols. People were neither wearing masks nor were they observing social distancing. India was slowly approaching the second wave of Covid which would hit us worse than the first wave.



Timeline of Covid vaccination in India
Vaccines were still in their clinical trials and weren’t available to the public. CoWIN platform was also under development. There was news of the availability of vaccines sometime in January 2021.
My Role
I was the lead designer on this project. I worked on the entire user experience. This project was completed under heavy urgency and the whole team helped each other out. I began with defining the brief, identifying possible problems and finding solutions. This was a huge project as it involved not only the product team but also the hospital team, on-ground staff and management.
A loud shout out to my team 🥳. View their names here!
Context
Variables:
Things we did not know
-
Price of the vaccine:
-
Will the price be variable across the nation?
-
-
Available Vaccines & their Dosage:
No. of doses per vaccine
-
Eligibility Criteria to get the vaccine:
-
Which age group would be initially vaccinated?
-
-
Vaccine Supply in Hospitals:
-
Would they have a sufficient vaccine supply?
-
No guarantee that a hospital will be active on certain days
-
-
Others:
-
CoWIN wasn’t developed yet - we did not have a point of reference
-
Basic rules like would we have the authority to issue vaccination certificates?
-
It was difficult to come up with a well-defined brief because government rules were being frequently changed, so we just rolled with whatever came our way!
Initial Problem Statement
-
Preparing to vaccinate a large number of people
-
Working in tandem with the government and not as competitors.
How we came up with our User Persona:
The next conundrum we faced was that of creating the user persona. We made a rough persona of the people who would use the government portal. We drew our persona in line with it - With the aim to expand the user group which could be vaccinated.

Government vaccine availing user persona:

-
Vacc. for the underprivileged
-
People of a certain age and co-morbidities
-
Incentive of free vaccine - to encourage the borderline sceptics
-
Walk-in candidates (as of 23 June, 2021 - 78% of vaccines had been administered via walk-in registration)
-
People w/o access to smartphones - could not access CoWIN

Our user persona:

-
People who were willing to pay
-
Willing to get vaccinated
-
Walk-in + Confirmed slots candidates
-
Had access to and knowledge of technology - tech savvy

Rest of the population:
Children under 18, people unwillling to get vaccinated, etc.
Enhanced user persona:

-
People who were willing to pay or could get sponsored
-
Willing to get vaccinated
-
Walk-in + wanted Confirmed slots
-
Had access to and knowledge of technology - tech savvy ( wanted confirmed slots)
-
Still did not know much about the vacc. process - need to keep them informed
Design Brief
Design a system for booking slots for a really large number of citizens (approx. 1lakh/day), in places with inefficient billing systems and where the amount to be billed is not clear until the user reaches the site of vaccination, where lines should move fast and the end product (vaccine availability) is not clear until the user reaches the counter on their turn.
Defining Success
We put down a few Success Metrics:

#1 Fewer on-ground staff:
#2 Facilitate fast-moving lines:
In an attempt to protect the people holding up the system it was important to ensure their safety. We had to build a system that wasn’t heavily dependent on people (who were at higher risk of getting infected).
Contamination was the biggest risk we were running. It was important that the lines kept moving as quickly as possible

#3 Prevent abuse of the system:
Resources (vaccines) were scarce. Also, there was a possibility that people might take advantage of the system. For example, use the same slot to vaccinate themselves and then reuse it to vaccinate a family member.
Tackling the problem
#1 Fewer on-ground staff

Tackling the problem
#2 Facilitate fast-moving lines:
Other than digitising major chunks of the whole process, we also tried to distribute the crowd.
We tried to divert the crowd from hospitals to other locations.
As a result:
-
Queues moved faster
-
Reduced the burden of vaccinating people on hospital staff

Hospital
Grounds

Private Grounds
(more controlled)
-
Office premises (Corporates):
Employees of respective companies were vaccinated on their office premises
-
Residential areas:
Plans to vaccinate societies/colonies within their premises
-
Walk-in candidates :
People w/o prior booking
-
Online candidates :
People with a slot booked via:-
Apollo247 app
-
CoWIN
-

Load on hospitals increasing queue size
Distributing load between
hospitals and private grounds
Tackling the problem
#3 Prevent abuse of the system (- Need for proof of billing):
The possible entry point for the foul play was between billing and just before vaccination. Both, the billing counter and the vaccination booth were never at the same location. They were often at different ends of the hospital. Once a billing slip was generated, it could be easily misused by multiple people to get the vaccine.
We brainstormed a couple of solutions:
#1 Indelible ink

We would mark each person who had paid and everyone with a mark on their finger would be eligible for the vaccine
The idea was discarded because:
Once the system was figured out people could fake a painted finger. Like in the elections it’s a great way to keep people (who have cast their vote) away but it would fail to move people from one stage to the other.
#2 Generating bills/invoices

Post payment we would generate a slip for each patient which would be deposited at the vaccination booth.
The idea was discarded because:
We knew that the printers at our hospitals wouldn’t be able to take the load of so many people.
-
Our printers were slow
-
Would slow down the queue
-
For offsite camps (private grounds) - our team would have to carry extra equipment - printers, ink, paper etc.
#3 QR codes

At the time of payment (offline or online), a link would be generated on the app. Additionally, an SMS would be sent to the patient’s registered phone number. The link would open a QR code and a special number. The QR code would then be scanned by SPOCs.
The idea was accepted because:
-
Easy and quick verification
-
Scanning doesn’t require extra equipment - everyone has a phone on them nowadays
-
Dual storage - Information would be stored both in the QR code as well as a special number shared via SMS
-
Reduced typing time - for generating bills
-
Queues would move faster
Final solutions included:
-
Booking tool:
-
In-app purchase (Prepaid)
-
Pay on site
-
Cashless (corporate-sponsored)
-
-
Informational services - Doc on call
-
Corporate Dashboard (cashless)
-
SPOC app (handled by my colleague)

Part 1
Addressing fear and scepticism
Around Jan 2021, Covid cases were on the rise. People were worried. There was news of vaccination being made available for 60+ people in the near future. But every piece of news added to the commotion.
We at Apollo realised that being a renowned hospital chain we should do something about it. We had an amazing group of doctors and we began answering people’s doubts and addressing their fears.
We opened communication lines & people could connect with our doctors and staff through call or chat.
Jan 2021
Before vaccination was open to the general public
#1
Trustable sources of information, a rich catalogue of content straight from Apollo hospital’s doctors
#2
Latest information about vaccine eligibility and important dates
#3
Call or chat with an Apollo Doctor (FREE of cost):
Those who were eligible for the upcoming vaccines wanted to know whether the vaccine would affect their comorbidities.
Mar 2021
After vaccination was open to 60+ and 45+ with co-morbidities
#1
Book slots
and get vaccinated at Apollo hospital
#2
Talk to doctors post-vaccination
about persisting symptoms
Trustable sources of information
Around Mar 2021 our booking tool was still under development at that time. So we released a quick fix.
We allowed customers to register for a slot. We allowed them to upload necessary documents so that the process on ground was simplified. Once their turn came, we would notify them over sms about the date of their vaccination. They could come to the site of vaccination, make the payment and get vaccinated.
A quick method to book a slot:
Apollo247 Homepage
Temporary method to book a vaccination slot

Part 2
Building a Vaccine Booking tool from scratch -
CoWIN was not in the picture yet!
Jan 2021
By January end the design of the booking tool was ready. Development was in progress.
Few on-ground problems were being tackled.
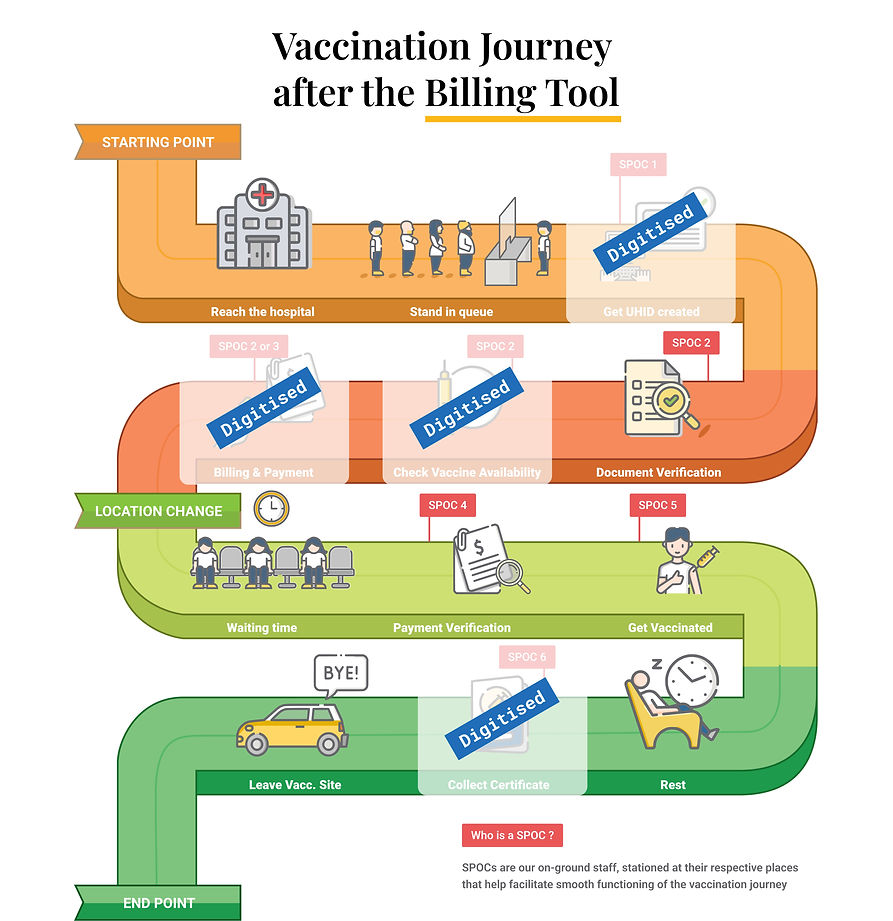
- include the on-ground steps that have been digitised to ensure that the queues move fast


Feb 2021
In Feb, we started facing troubles around the payment side.
Part 3a: Online Payment issues
#Difficulty in making online payments
The problem was twofold:
-
Tech constraints (Minor issue):
Due to this, we were unable to process online payments
-
Vaccine availability issue despite prepayment (Major issue):
It is very difficult to explain to a paying customer that the vaccine that they had requested is now out of stock.
-
Each hospital had to cater to both walk-in candidates (people without a slot) and prepaid customers. We could not reserve vaccines only for prepaid customers - hence no guarantee of the chosen vaccine.
-
In case verification of documents failed - the prepaid customer would not be vaccinated that day - their money would be refunded but they would have to go through the booking process all over again
-
Vaccine prices varied - In case of unavailability of one vaccine, we could provide an alternative but:
-
The patient may not want that vaccine
-
In case the patient agrees, we would have to either return the patient’s money or charge him extra - all the explanations of alternate vaccines and exchange of money would further hold up the queue
-
-
Brainstorming
We brainstormed a few ways to go about inoculating people without making upfront payment holding up the line. In the absence of references we looked up several analogous systems:
#1 Tatkal booking system of the Indian railways:
Everybody pays (even those with a waitlisted ticket) and if they don’t get a confirmed seat - money was refunded. Eg: TDR or refund at a separate counter
#2 Food Court:
#Create Bank Mandates:
Fill a physical card with money. Use the money and get the remaining money refunded on your way out.
Money stays in the person’s account but gets blocked. It is debited only if the person gets a confirmed slot at the time of vaccination.
#4 Cashless lanes (collaborating with Corporates):
We joined hands with corporates who wanted to help get their employees vaccinated. As a result, the whole payment system was not needed for such candidates. We just calculated the people that were vaccinated and the type of vaccine and the companies paid for it later.

Mid Feb 2021
Around mid Feb, work was started around the Corporate dashboard and onboarding
Part 3b
Cashless lanes -Vaccination for employees, sponsored by their companies
#2 Onboarding - Employee Verification of & UHID Creation
A personalised link was emailed to each eligible employee. On clicking the link they were taken through the onboarding process.
#1 Click the link received on the employee’s email
May 2021
The corporate dashboard became functional around the time when vaccination was opened to all residents above the age of 18
#3 Dashboard - Exploring benefits
#1 Package Deal:
Along with the vaccination slot came a lot more benefits for the well being of the employee
#2 Expectation setting:
Informing the user what to expect during their vaccination journey
#3 Nudge:
#3 Nudge:
#4 FAQs:
A list of the frequently asked questions
End of May 2021:
Around 23 May our payment system was up and running. We were taking retail bookings (non-corporate) as well as bookings for dependents
Visible on the day of vaccination
Once vaccination was completed
If the appointment was cancelled. Eg. document verification failed
Once documents were verified
3 Visible statuses:
Book vaccine through the booking tool

End of May 2021:
Integration with CoWIN
Integration with CoWIN was compulsory once CoWIN was launched. But CoWIN came into the picture later. Quite a few vaccinations had been conducted without CoWIN.
When we rolled out vaccinations to the public we prompted the patient to register on CoWIN. But a lot of people did not bother to register. Because the CTA would take them to the CoWIN website - where they would have to fill in their details all over again.
Later, we made it a two-step process. On clicking the CTA - the patient would have to verify their phone number - after which we would retrieve their details. If they were already registered on CoWIN we would link it. Otherwise, we would create an account on their behalf.
Integration with CoWIN:
Impact
appreciation & other learnings
We have vaccinated employees of
We are now vaccinating in:
285
-
33 cities across the country
-
109 hospital sites
corporates
Appreciation from Corporates (Apple, India)

Things I learnt:
-
In the absence of a design brief, you build on what you already know:
We heavily relied on analogous systems. We studied them and picked up parts that could be beneficial to us. -
Multiple reviews from the same people may lead to identical feedback (most of the time) but reviews from cross-functional teams lead to useful insights:
We showed the prototype not just to the product team (PMs and tech) but also to the on-ground staff, doctors and all the heads. We got insights like we had inkjet printers at the hospitals which won't be able to take the kind of load we were expecting. -
One cannot foresee the future, so cross the bridge when you come to it:
Initially, parking became a problem - due to Covid, people wanted to avoid travelling by public transport or on 2-wheelers. Further disregard for slot schedules led to too many four-wheelers on the hospital campus. Eventually, people understood we were following the slots, so they started following it too.
Shout out to my entire team that made this project possible 🥳
Product team:
Ajay
Bhagath
Arpit
Prashant
Design:
Divya - who worked on the app for SPOCs
Dev & QA team:
Pankaj Goel
Prabhat
Gufran
Rahul K
Gowthami
Shikha
Vasudev
Vamsi
Ashish
Chandrashekhar
Asad